
Sun et al. "Increased emergency cardiovascular events among under-40 population in Israel during vaccine rollout and third COVID-19 wave": vaccine-induced undetected severe cardiovascular side effects
by Paul Alexander
Dr. Ramin Oskoui shared: OMINOUS, regarding vaccine-induced undetected severe cardiovascular side-effects and underscore the already established causal relationship between vaccines and myocarditis
Great sharing by Dr. Oskoui out of Washington. This study is powerful for it allows a glimpse at the Israeli data but prior to the pandemic, during the first 2 waves with no vaccine, and the third wave coincident with the vaccine roll out. It is not causal so to speak but punishingly close.
SOURCE:
Key issues:
A retrospective population-based study leverages the IEMS data system and analyzes all calls related to CA and ACS events over two and a half years, from January 1st, 2019, to June 20th, 2021.
“it allows to study how CA and ACS call counts change over time with different background conditions and potentially highlight factors that are associated with the observed temporal changes…”
“The study’s dataset includes all non-cancelled calls with reported patient age and a verified call-type of either CA or ACS. CA calls were defined as a sudden electrical malfunction of the heart of presumed cardiac or medical etiology, resulting in collapse of a patient, excluding CAs related to trauma, drug overdose, or suicide. ACS calls were defined as conditions where the patients experience a reduction in blood flow to the heart that is associated with myocardial infarction.”
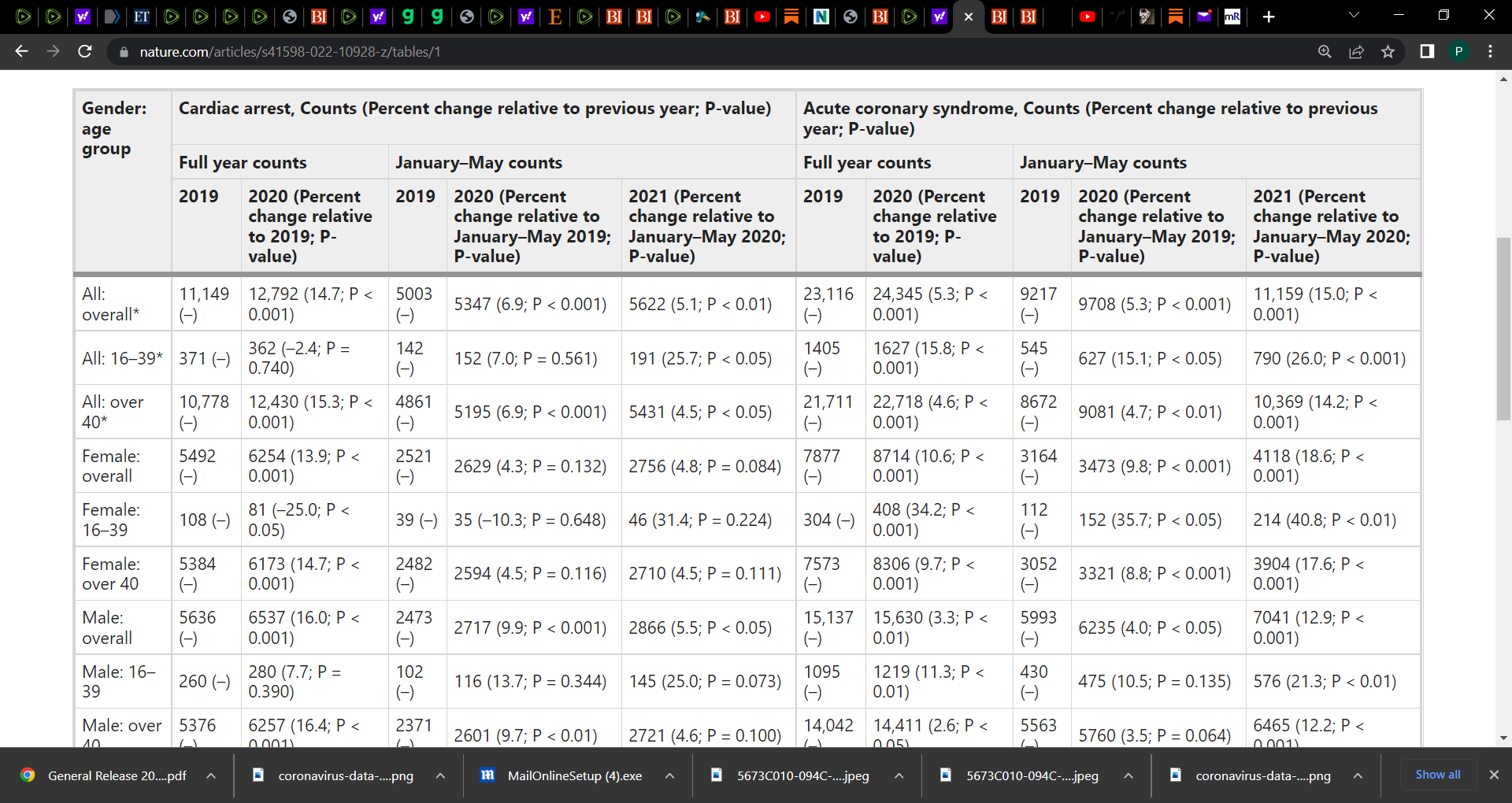
Key table of results (Table 1):
See Figure 1 and the surge in cardiac events linked to the 1st and 2nd shot.
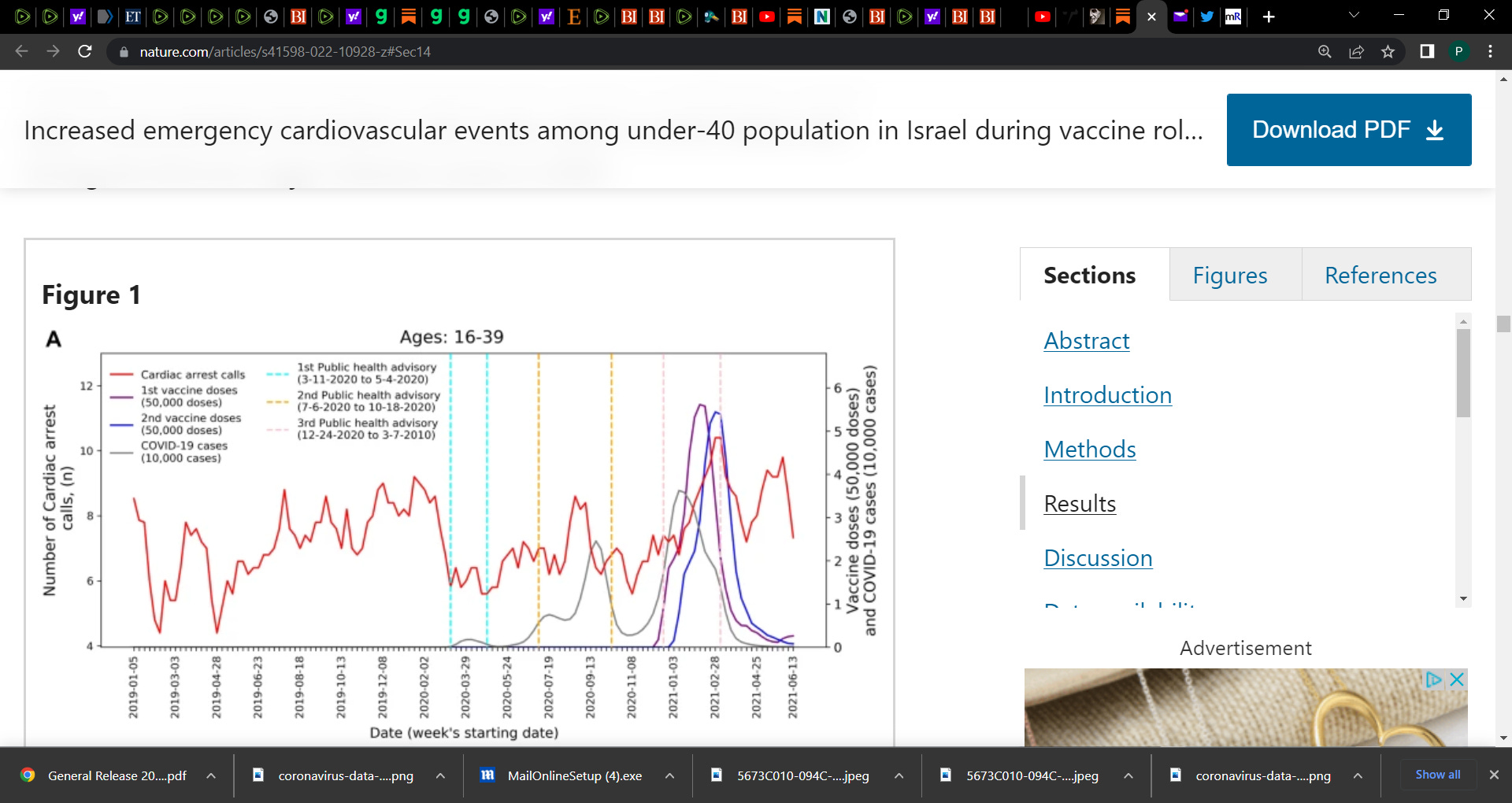
Researchers found an increase of over 25% in both call types during January–May 2021, compared with the years 2019–2020.
“Using Negative Binomial regression models, the weekly emergency call counts were significantly associated with the rates of 1st and 2nd vaccine doses administered to this age group but were not with COVID-19 infection rates. While not establishing causal relationships, the findings raise concerns regarding vaccine-induced undetected severe cardiovascular side-effects and underscore the already established causal relationship between vaccines and myocarditis, a frequent cause of unexpected cardiac arrest in young individuals. Surveillance of potential vaccine side-effects and COVID-19 outcomes should incorporate EMS and other health data to identify public health trends (e.g., increased in EMS calls), and promptly investigate potential underlying causes.”
Note, you must consider the limitations and major is the fact that this is aggregated data that lacks any information on the patients. We needed more granular data. This is important to factor in as you draw conclusions. For example, what were the comorbidities? How ill were the persons? What was the status in terms of verified COVID infected status and also, what was the vaccine status. It is not clear in my reading. We needed a bit more details to judge if the vaccine is the underpinning contributor to the increased calls etc. but nonetheless, this study is potent and adds another dimension to the debate on the lethality of the mRNA platform.