'XBB.1.5' is the new United States grand-daddy sub-variant now displacing BQ.1.1 & BQ.1 & BA.5; XBB.1.5 based on CDC data today accounts for 40.5% proportion; Vanden Bossche, Hodkinson, I, we warned
by Paul Alexander
that the virus has become largely resistant to the induced vaccinal antibodies (Ab) & the non-neutralizing Abs place sub-optimal immune pressure on the antigen while infection is high; drives variants
The pace at which XBB.1.5 is (has) supplanting (supplanted) BA.5 and BQ.1.1 etc. is staggering. Moreover, indications are that it is the vaccine that is driving the variants (Fantini et al., Liu et al.), not the virus. Yes, viruses mutate readily and spontaneously (due to the unstable genetic copying mechanism etc.) yet it is the added pressure by the vaccinal antibodies (sub-optimal immune pressure due to immature undeveloped antibodies) on the infectiousness of this virus, that is, on the epitopes/receptor binding domain as well as the N-terminal domain (and others). That ‘selection pressure’ is driving the emergence of variants.
They have designed the roll-out, the vaccine, all of it to never end. That this so called ‘pandemic’ will never end; Fauci, Bourla, Bancel, Francis Collins, Walensky, CDC, NIH, FDA et al., they all know that as long you mass vaccinate a population (massively and rapidly) across all age-groups and keep injecting while there is massive circulating virus (massive infectious pressure by the circulating virus), using a gene injection (vaccine) that does not sterilize (neutralize) the virus (stop infection or replication or transmission), then natural selection pressure will select for the ‘fittest’, most ‘hardiest’, most infectious variants that could overcome that sub-optimal pressure, infect, proliferate, become enriched in the environment, and go on to become the new dominant sub-variant, case in point, XBB.1.5. XBB.1.5 is now replacing BA.5 and BQ.1.1 (based on CDC reporting) as the prior dominant sub-variant. There will be viral immune escape, original antigenic sin, and antibody-dependent enhancement of infection (and/or disease), as well as now emerging indications of immune tolerance (based on IgG4 class switching), in this case, due to the interplay and dynamics between the virus and the host immune system. You cannot discuss one without the other.
This pandemic is designed to never end for 100 years. With this fraud gene injection ‘slow kill’ bioweapon. If I wanted to design a bioweapon to slow kill people, I would design this very vaccine and roll it out in the very manner it has been since January 2021. IMO. This gene injection behaves like a bioweapon. So either the injection must be stopped or the infectious pressure must be reduced. There is no end in sight once we keep injecting and it is the vaccine that is causing the variants to emerge. Not the virus. The vaccinal antibodies are giving the virus infectious properties it prior did not have. The result in the vaccinee is becoming infected, sick, and dying.
You want the variants to stop, then stop the COVID gene injection. Moreover, if you do not stop, there is the risk of a more virulent strain potentially emerging that could decimate humanity. Infectious and more virulent/lethal.
New sub-variant chart:
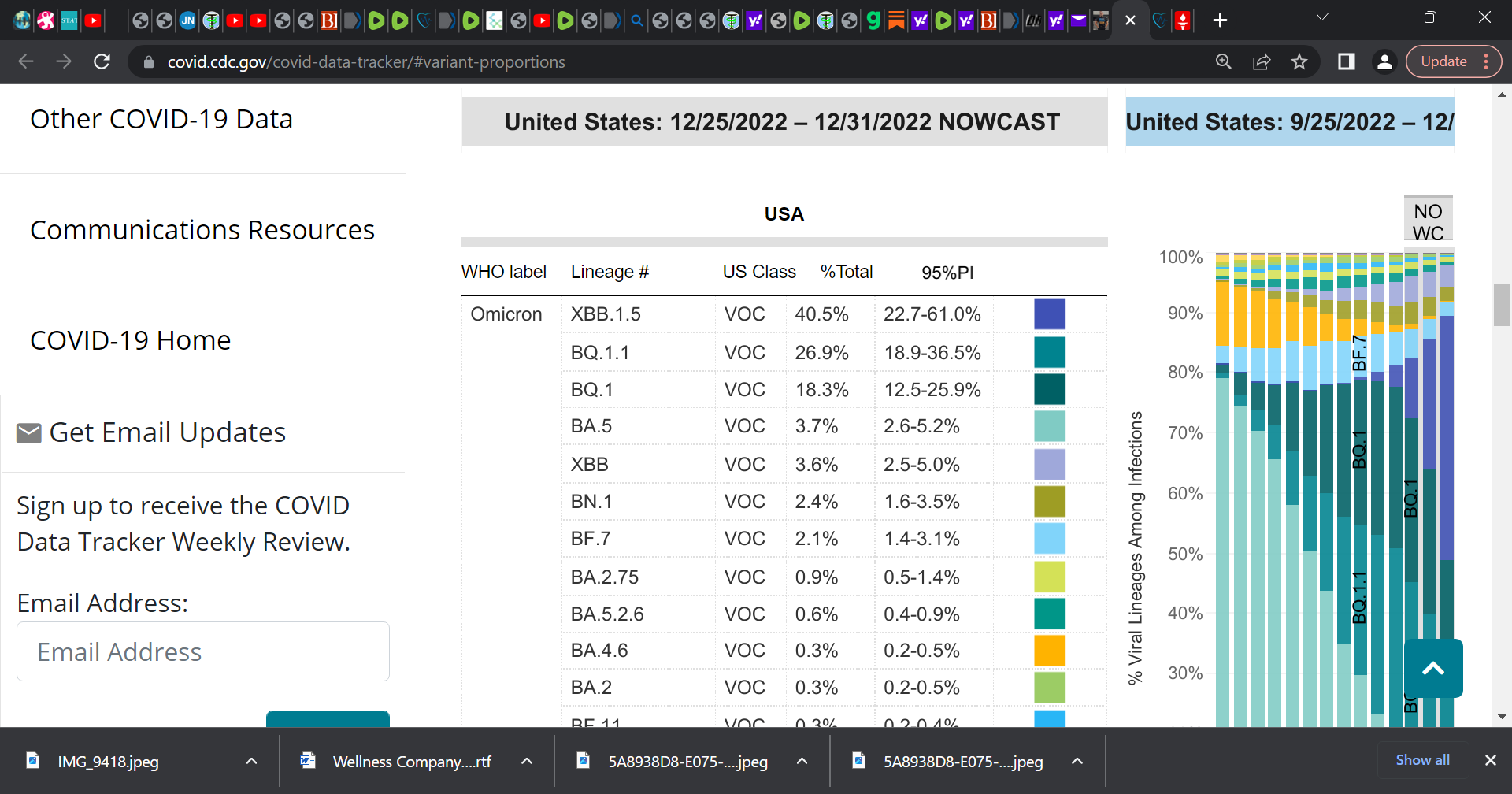
SOURCE: https://covid.cdc.gov/covid-data-tracker/?utm_source=substack&utm_medium=email#variant-proportions
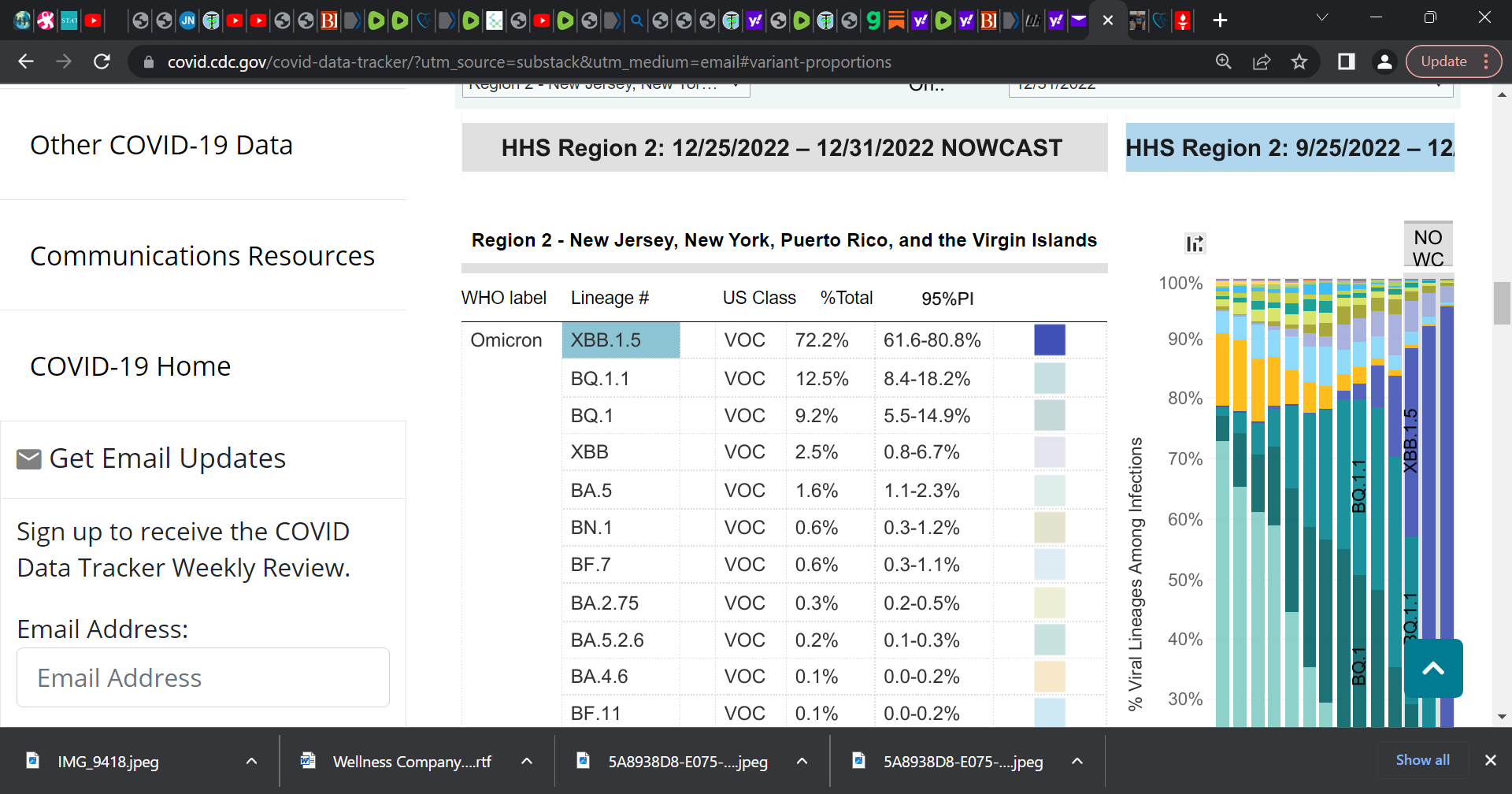
Just look at New York, New Jersey etc. region 2, it accounts for 75% of porportion:
Similarly, Region 1, XBB.1.5 is 75%.
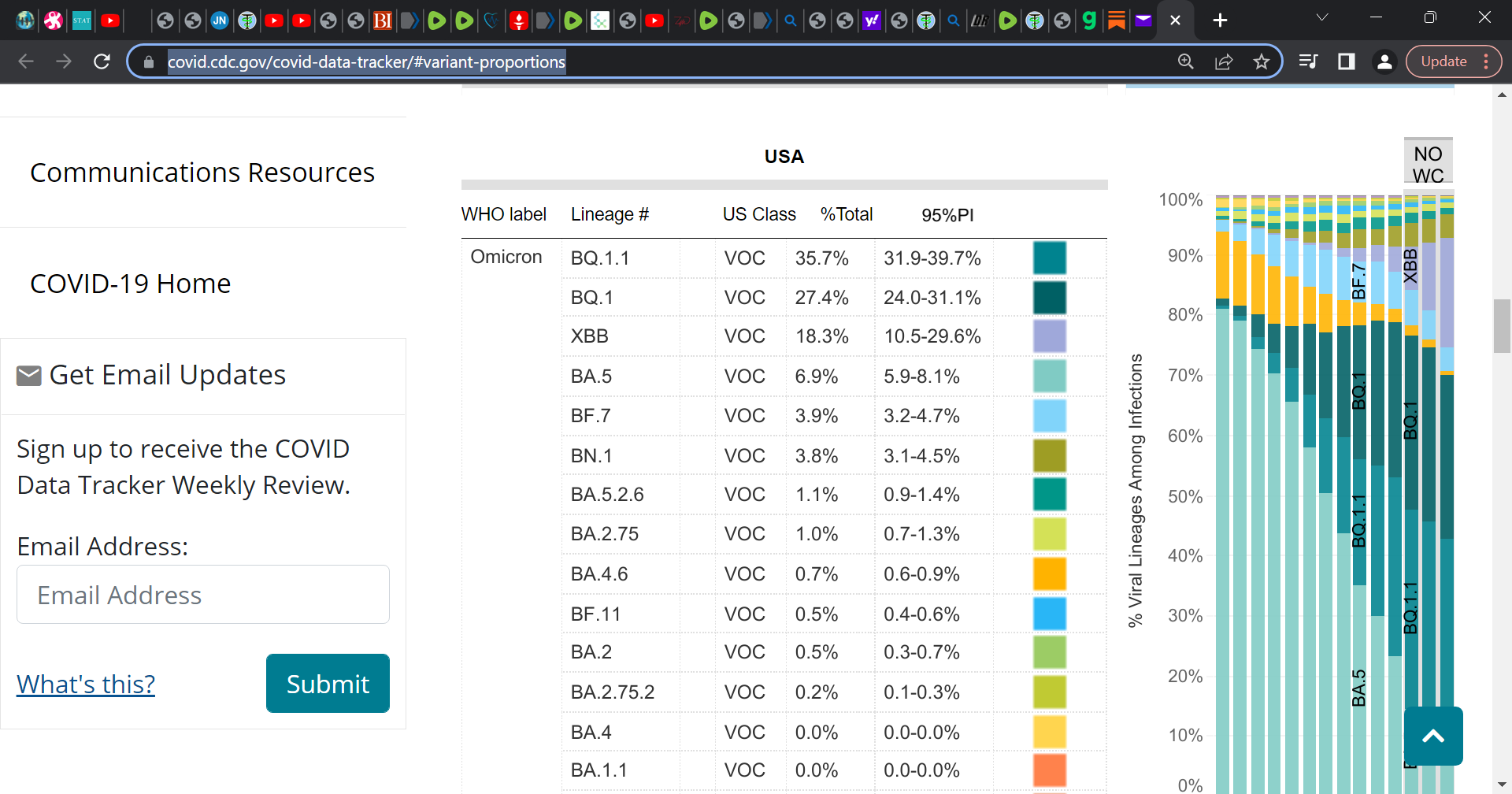
Last sub-variant chart that I posted: