
Natural immunity wins AGAIN!! Patalon et al.: pre-print "Naturally-acquired Immunity Dynamics against SARS-CoV-2 in Children and Adolescents'
by Paul Alexander
Children and adolescents who were previously infected with SARS-CoV-2 remain protected against reinfection; Policy decision makers should consider if prior-infected children & adolescents to be vaxxed
This Israeli study reveals exceptional long-lasting immunity post infection in children, and particularly in 5-11 year olds.
SOURCE:
Naturally-acquired Immunity Dynamics against SARS-CoV-2 in Children and Adolescents
para ‘A retrospective study using a matched test-negative case control design and a retrospective cohort design.
Setting: Nationally centralized database of Maccabi Healthcare Services, an Israeli national health fund that covers 2.5 million people.
Participants: The study population included between 293,743 and 458,959 individuals (depending on the model), 5-18 years of age, who were unvaccinated SARS-CoV-2 naive persons or unvaccinated convalescent patients.
Evaluated three SARS-CoV-2-related outcomes: (1) documented PCR confirmed infection or reinfection, (2) COVID-19 and (3) severe COVID-19.
Results: Overall, children and adolescents who were previously infected acquired durable protection against reinfection (symptomatic or not) with SARS-CoV-2 for at least 18 months. Importantly, no COVID-19 related deaths were recorded in either the SARS-CoV-2 naive group or the previously infected group. Effectiveness of naturally-acquired immunity against a recurrent infection reached 89.2% (95% CI: 84.7%-92.4%) three to six months after first infection, mildly declining to 82.5% (95% CI, 79.1%-85.3%) nine months to one year after infection, then remaining rather steady for children and adolescents for up to 18 months, with a slight non-significant waning trend. Found that ages 5-11 exhibited no significant waning of naturally acquired protection throughout the outcome period, whereas waning protection in the 12-18 age group was more prominent, but still mild.
Conclusions: Children and adolescents who were previously infected with SARS-CoV-2 remain protected against reinfection to a high degree and policy decision makers should consider when and if convalescent children and adolescents should be vaccinated.’
Some additional information:
Recall this study by Dorabawila et al. Effectiveness of the BNT162b2 vaccine among children 5-11 and 12-17 years in New York after the Emergence of the Omicron Variant and key findings, “in the Omicron era, the effectiveness against cases of BNT162b2 declined rapidly for children, particularly those 5-11 years.”
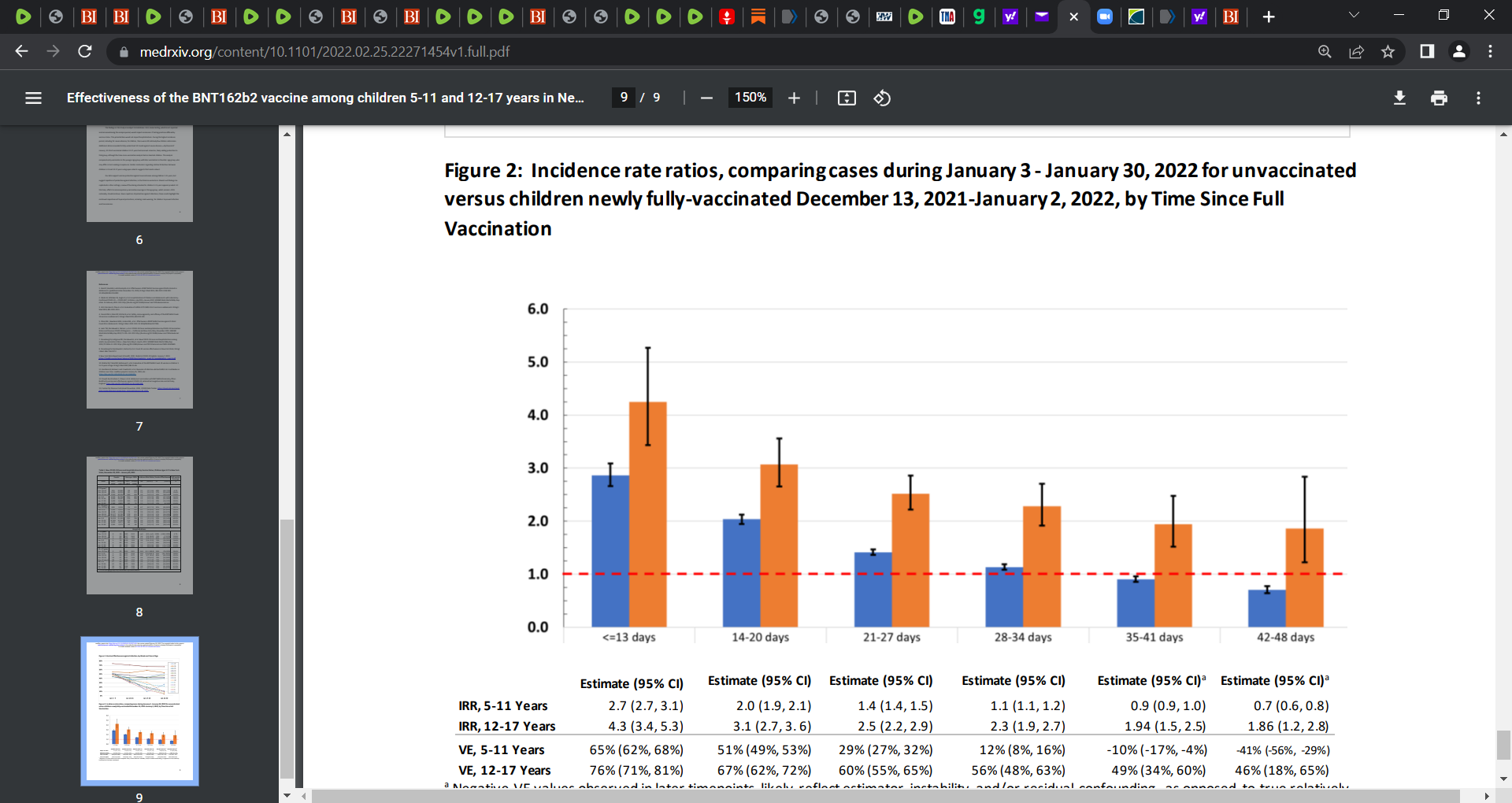
“From December 13, 2021 to January 30, 2022, among 852,384 fully-vaccinated children 12-17 years and 365,502 children 5-11 years, VE against cases declined from 66% (95% CI: 64%, 67%) to 51% (95% CI: 48%, 54%) for those 12-17 years and from 68% (95% CI: 63%, 72%) to 12% (95% CI: 6%, 16%) for those 5-11 years. During the January 24-30 week, VE for children 11 years was 11% (95%CI -3%, 23%) and for those age 12 was 67% (95% CI: 62%, 71%).
VE against hospitalization declined changed from 85% (95% CI: 63%, 95%) to 73% (95% CI: 53%, 87%) for children 12-17 years, and from 100% (95% CI: -189%, 100%) to 48% (95% CI: -12%, 75%) for those 5-11 years. Among children newly fully-vaccinated December 13, 2021 to January 2, 2022, VE against cases within two weeks of full vaccination for children 12-17 years was 76% (95% CI: 71%, 81%) and by 28-34 days it was 56% (95% CI: 43%, 63%). For children 5-11, VE against cases declined from 65% (95% CI: 62%, 68%) to 12% (95% CI: 8%, 16%) by 28-34 days.”
Remember Föhse et al. showed us the evidence of vaccine-induced disturbance of both innate and adaptive immune responses.
SOURCE:
Föhse et al.: The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses
Researchers confirmed that BNT162b2 (Pfizer) vaccination of healthy individuals induced effective humoral and cellular immunity against several SARS-CoV-2 variants. “The BNT162b2 vaccine also modulated the production of inflammatory cytokines by innate immune cells upon stimulation with both specific (SARS-CoV-2) and non-specific (viral, fungal and bacterial) stimuli. The response of innate immune cells to TLR4 and TLR7/8 ligands was lower after BNT162b2 vaccination, while fungi-induced cytokine responses were stronger. In conclusion, the mRNA BNT162b2 vaccine induces complex functional reprogramming of innate immune responses”…
SOURCE:
Seneff et al.: Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs
“The mRNA SARS-CoV-2 vaccines were brought to market in response to the public health crises of Covid-19. The utilization of mRNA vaccines in the context of infectious disease has no precedent. The many alterations in the vaccine mRNA hide the mRNA from cellular defenses and promote a longer biological half-life and high production of spike protein. However, the immune response to the vaccine is very different from that to a SARS-CoV-2 infection. In this paper, we present evidence that vaccination induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health. Immune cells that have taken up the vaccine nanoparticles release into circulation large numbers of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites. We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance. These disturbances potentially have a causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell's palsy, liver disease, impaired adaptive immunity, impaired DNA damage response and tumorigenesis. We show evidence from the VAERS database supporting our hypothesis. We believe a comprehensive risk/benefit assessment of the mRNA vaccines questions them as positive contributors to public health.”
SOURCE:
Follmann et al.: Anti-nucleocapsid antibodies following SARS-CoV-2 infection in the blinded phase of the mRNA-1273 Covid-19 vaccine efficacy clinical trial
‘N-antibodies were seen in only 40% of those infected after vaccination, compared with 93% of those infected after placebo. Among participants with PCR-confirmed Covid-19 illness, seroconversion to anti-N Abs at a median follow up of 53 days post diagnosis occurred in 21/52 (40%) of the mRNA-1273 vaccine recipients vs. 605/648 (93%) of the placebo recipients (p < 0.001).’