
U.K. Health Security Agency first “COVID-19 vaccine surveillance report” of 2022, which collates infection rate data for the final weeks of 2021 (weeks 49-52); a DEVASTATING REPORT
by Paul Alexander
See TABLE 13, page 42, these are case rates per 100,000 divided by age group & vaccination status; shows vaccine is a failure and no case for mandates; see Danish study (vaccine drives OMICRON spread)
First, huge hugs and love to all!
Two key papers are presented here and some calculations:
-
U.K. Health Security Agency first “COVID-19 vaccine surveillance report” of 2022
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1045329/Vaccine_surveillance_report_week_1_2022.pdf
AND
-
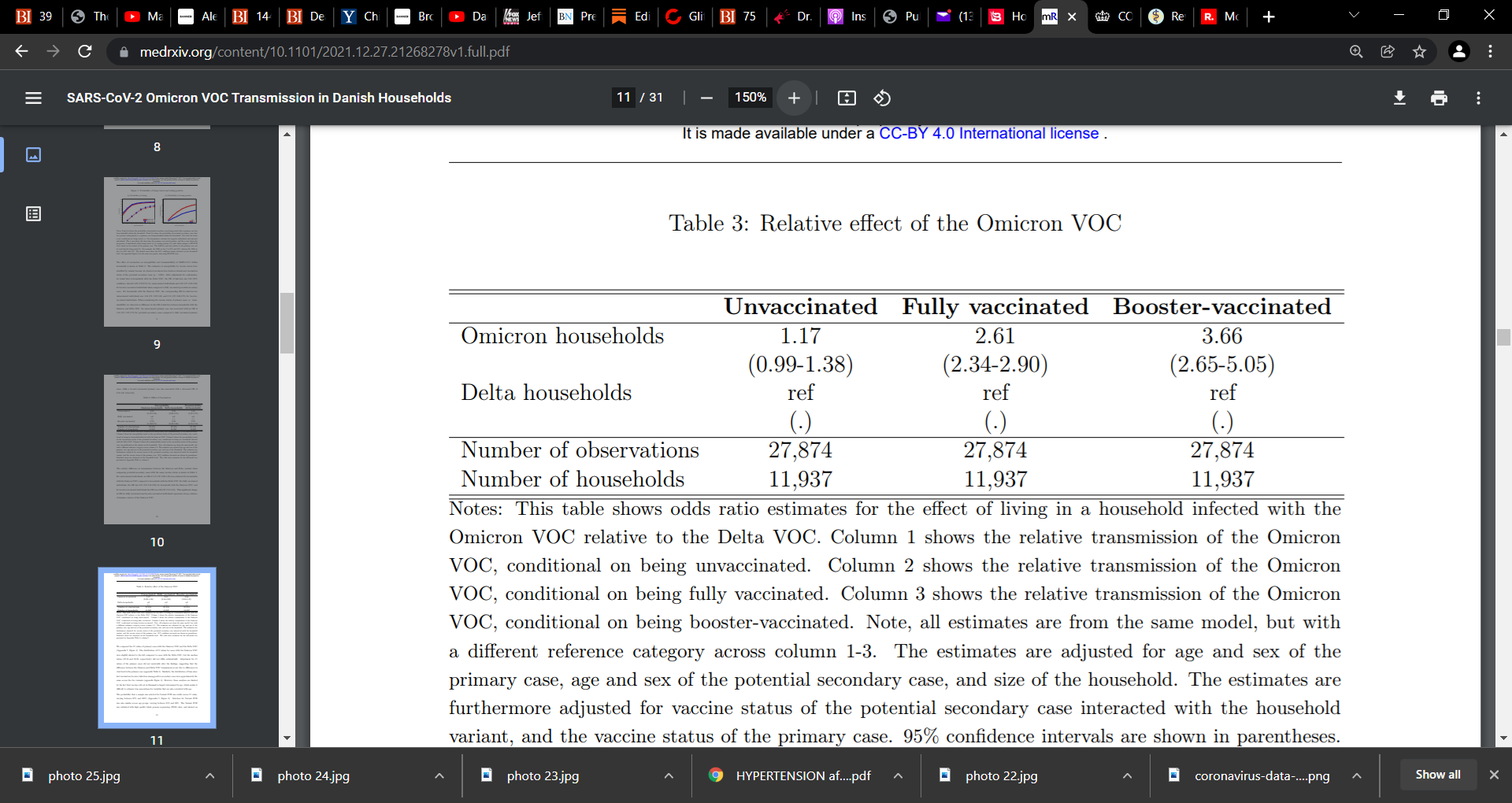
SARS-CoV-2 Omicron VOC Transmission in Danish Households
https://www.medrxiv.org/content/10.1101/2021.12.27.21268278v1.full
-
See also 6 studies at the end of this stack on OMICRON to evidence the failure
Table 13, page 42 key columns of the UK report:
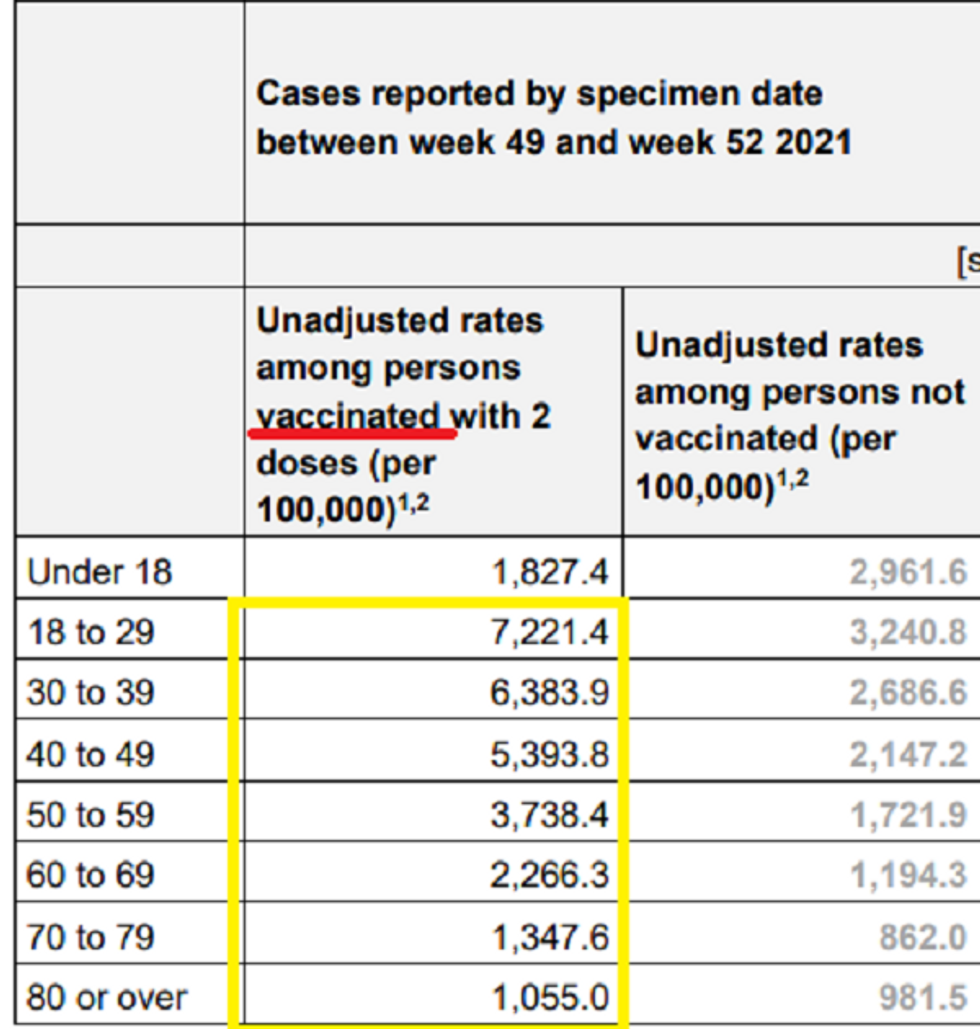
UK has given us clear, detailed, granular data all along, better than all other nations.
It is clear from above that the vaccinated is being infected at far greater levels than the unvaccinated. Except < 18 years old. This is disastrous. We have to urgently study the extent that they can transmit to both vaccinated and unvaccinated persons, and how much they can get sick.
I have computed the vaccine efficacy in the following table and see all 18 years old and above, they are all significantly negative…this is catastrophic for the vaccine in the era of OMICRON….
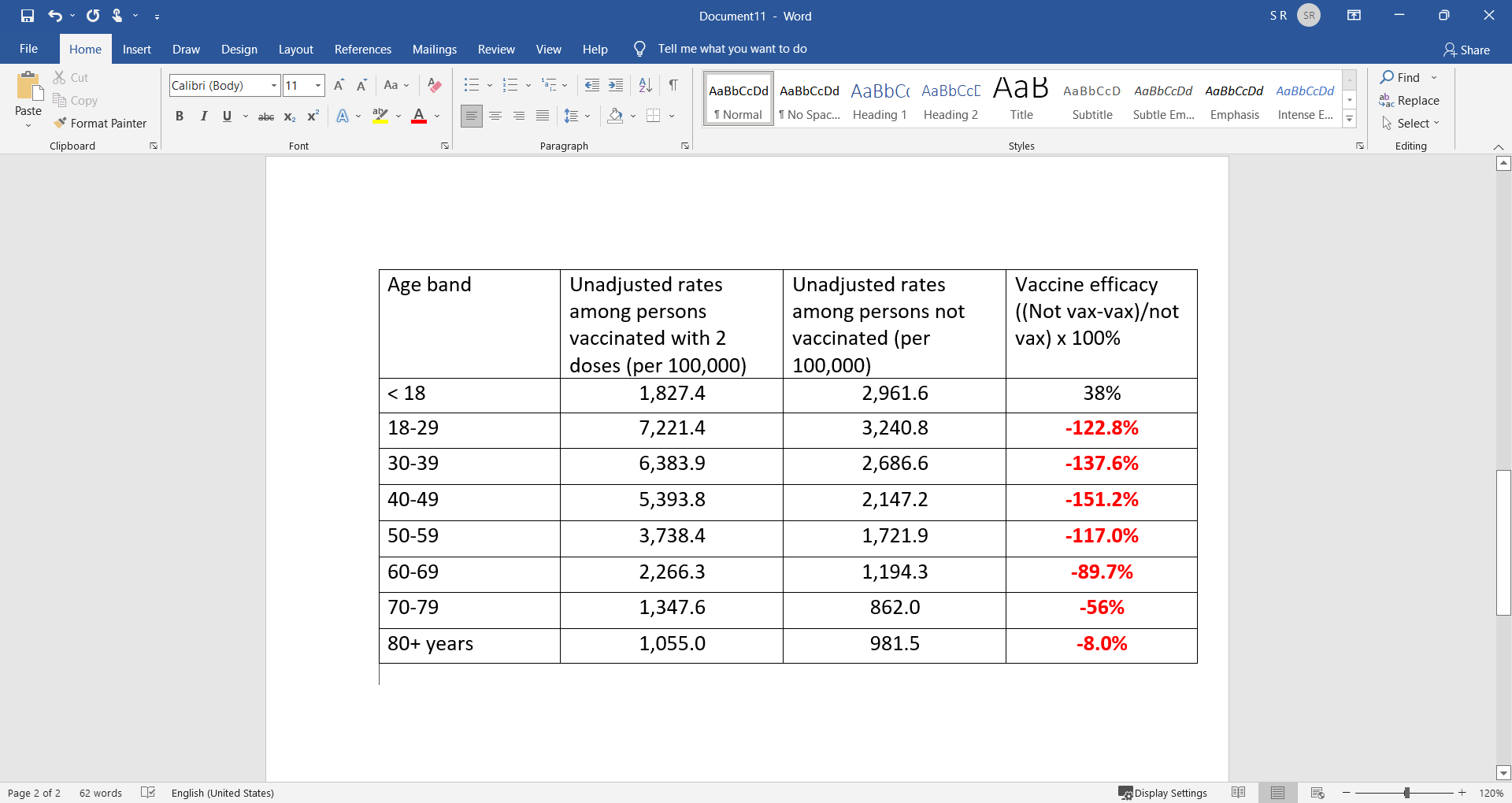
It is seen in the above table that there is clear negative efficacy of the vaccines as to risk of being infected. This captures OMICRON. The vaccine negative efficacy appears to come fast, in a month or so.
This raises what I and we have been saying in our substacks here, that the vaccine during this pandemic with circulating virus, is driving infection and variants. It is the vaccinated that is most at risk. The vaccine is driving viral immune escape. It is the combination of infectious pressure and sub-optimal immune pressure from mounting antibodies, using mass vaccination, that is driving natural selection but also the immune escape that is causing the vaccinated to be infected.
Unvaccinated persons are not mounting antibodies and it is hard to see how they place the virus under immune pressure. It is the suboptimal immune pressure from the vaccine that is at play here pressuring the virus. What say you?
There is also decent theory that it is the initial prime/exposure of the immune system with vaccine (1st shot) that has primed the immune system to respond with systemic antibodies with each exposure (e.g. to the repeat boosters) and not the correct cytotoxic NK cellular response at the local respiratory site of infection. Thus the immune system response is wrong, and thus the vaccinated is getting more and more infected in the respiratory tract and deeper into the lungs as the wrong soldiers (antibodies) are being sent to the wrong site e.g. blood.
This also lines up very good with a study in Denmark looking at OMICRON secondary transmission in Danish Households.
SARS-CoV-2 Omicron VOC Transmission in Danish Households
https://www.medrxiv.org/content/10.1101/2021.12.27.21268278v1.full
See table 3, page 11 here…vaccines are causing the super-spreading of Omicron in the homes, but we can infer everywhere. Yes, there is immune escape, but the vaccine is lighting a fire…we actually see a dose response. Some argue it could be the immune system is suppressed post vaccine but we are really talking about secondary transmission here and there appears to be a clear link with vaccine and more vaccine at that.
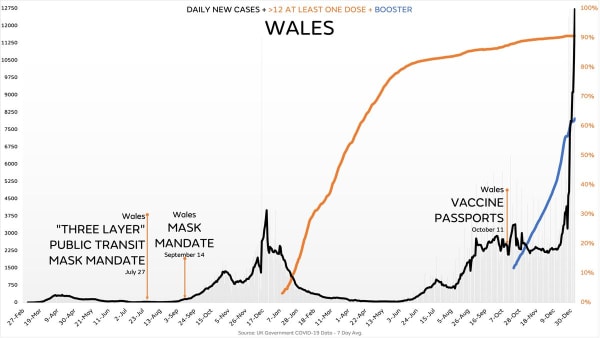
Look at this chart of Wales...has mask mandates and passports and 3rd booster….see their infection rates….


See 6 OMICRON related studies:
1) Wilhelm et al. reported on reduced neutralization of SARS-CoV-2 omicron variant by vaccine sera and monoclonal antibodies. “in vitro findings using authentic SARS-CoV-2 variants indicate that in contrast to the currently circulating Delta variant, the neutralization efficacy of vaccine-elicited sera against Omicron was severely reduced highlighting T-cell mediated immunity as essential barrier to prevent severe COVID-19.”
2) CDC reported on the details for 43 cases of COVID-19 attributed to the Omicron variant. They found that “34 (79%) occurred in persons who completed the primary series of an FDA-authorized or approved COVID-19 vaccine ≥14 days before symptom onset or receipt of a positive SARS-CoV-2 test result.”
3) Dejnirattisai et al. presented live neutralisation titres against SARS-CoV-2 Omicron variant, and examined it relative to neutralisation against the Victoria, Beta and Delta variants. They reported a significant drop in “neutralisation titres in recipients of both AZD1222 and BNT16b2 primary courses, with evidence of some recipients failing to neutralise at all.”
4) Cele et al. assessed whether Omicron variant escapes antibody neutralization “elicited by the Pfizer BNT162b2 mRNA vaccine in people who were vaccinated only or vaccinated and previously infected.” They reported that Omicron variant “still required the ACE2 receptor to infect but had extensive escape of Pfizer elicited neutralization.”
5) Holm Hansen et al.’s Denmark study looked at vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series. A key finding was reported as “VE against Omicron was 55.2% initially following primary BNT162b2 vaccination, but waned quickly thereafter. Although estimated with less precision, VE against Omicron after primary mRNA-1273 vaccination similarly indicated a rapid decline in protection. By comparison, both vaccines showed higher, longer-lasting protection against Delta.” In other words, the vaccine that has failed against Delta is even far worse for Omicron. The table and figure below paint a devastating picture. See where the green dot is (Omicron variant) in the vertical lines (blue is Delta) and the 2 edges of the bars (upper and lower lips) 91 days out for Omicron (3 months). Both Pfizer and Moderna show negative efficacy for Omicron at 31 days (both are below the ‘line of no effect’ or ‘0’). The comparative table is even more devastating for it shows how much less vaccine effectiveness there is for Omicron. For example, at 1-30 days, Pfizer showed 55.2% effectiveness for Omicron versus 86.7% for Delta, and for the same period, Moderna showed 36.7% effectiveness for Omicron versus 88.2% for Delta.
6) UK reporting showed that boosters protect against symptomatic COVID-19 caused by Omicron for about 10 weeks; the UK Health Security Agency reported protection against symptomatic COVID-19 caused by the variant dropped from 70% to 45% following a Pfizer booster for those initially vaccinated with the shot developed by Pfizer with BioNTech. Specifically reporting by the UK Health Security Agency showed “Among those who received an AstraZeneca primary course, vaccine effectiveness was around 60% 2 to 4 weeks after either a Pfizer or Moderna booster, then dropped to 35% with a Pfizer booster and 45% with a Moderna booster by 10 weeks after the booster. Among those who received a Pfizer primary course, vaccine effectiveness was around 70% after a Pfizer booster, dropping to 45% after 10-plus weeks and stayed around 70 to 75% after a Moderna booster up to 9 weeks after booster.”