
Week 10 COVID data UK, up to 6 March, shows continuing negative efficacy, with > 18 years showing higher infection; compared to week 9; key is the potent role of INNATE immune system
by Paul Alexander
Pay attention to the potential role of the INNATE immune system in both the vaccinated and unvaccinated in the evolutionary dynamics (infectious pressure, immune pressure on the spike, the virus)
We see negative efficacy again, and the role of original antigenic sin (I call it ‘mortal’ antigenic sin) and AMVE/ADE (antibody mediated viral enhancement).
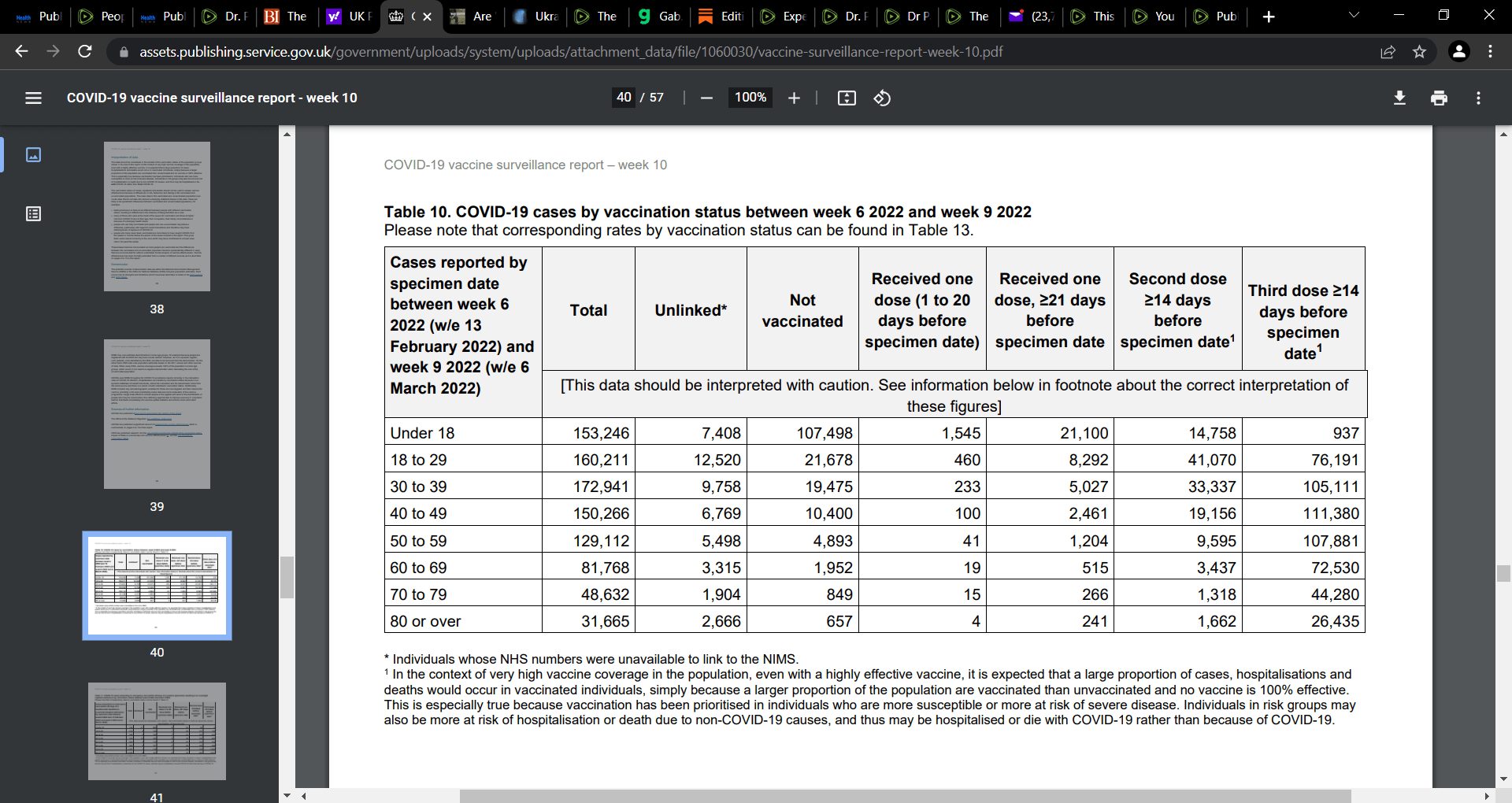
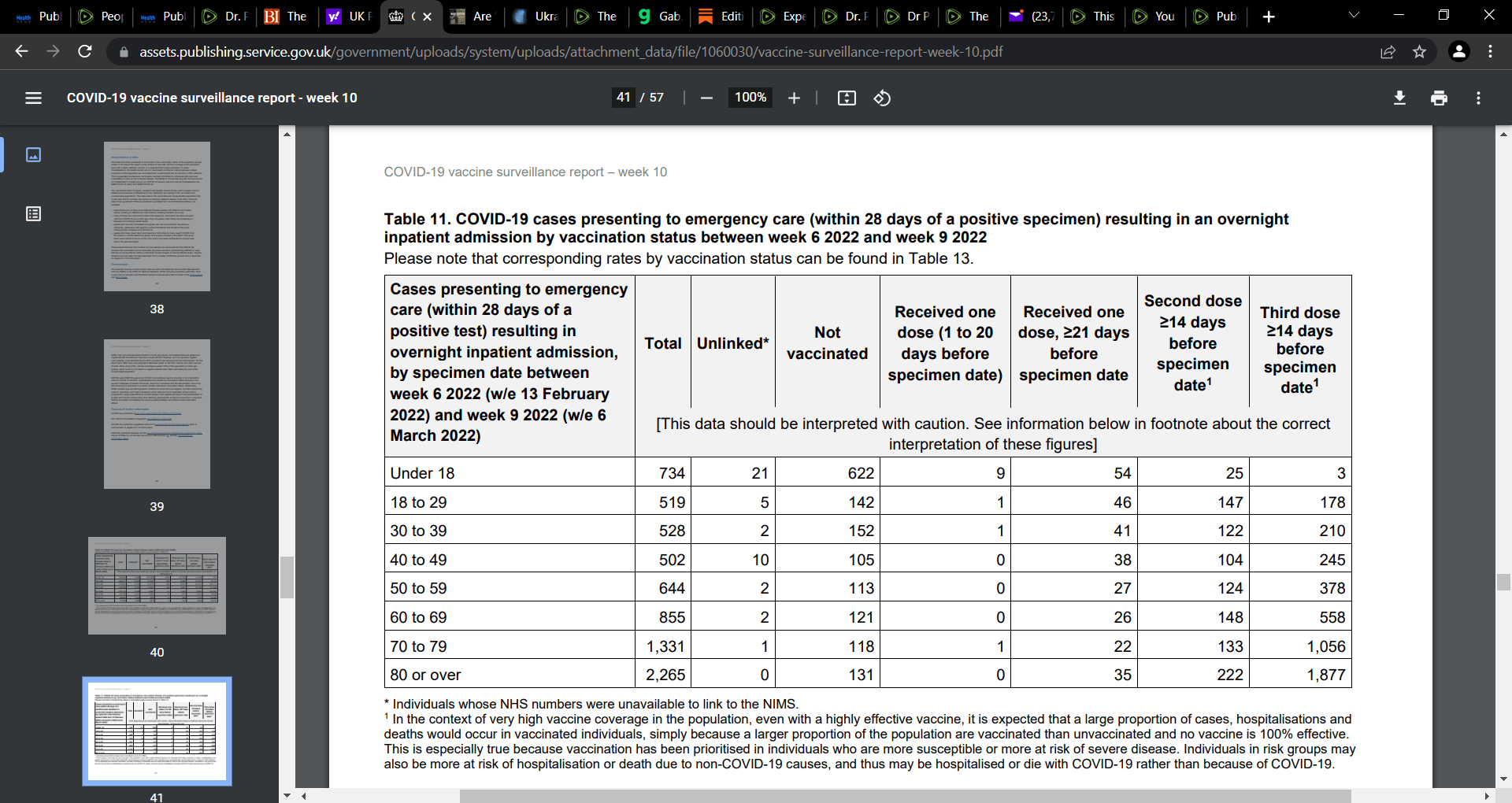
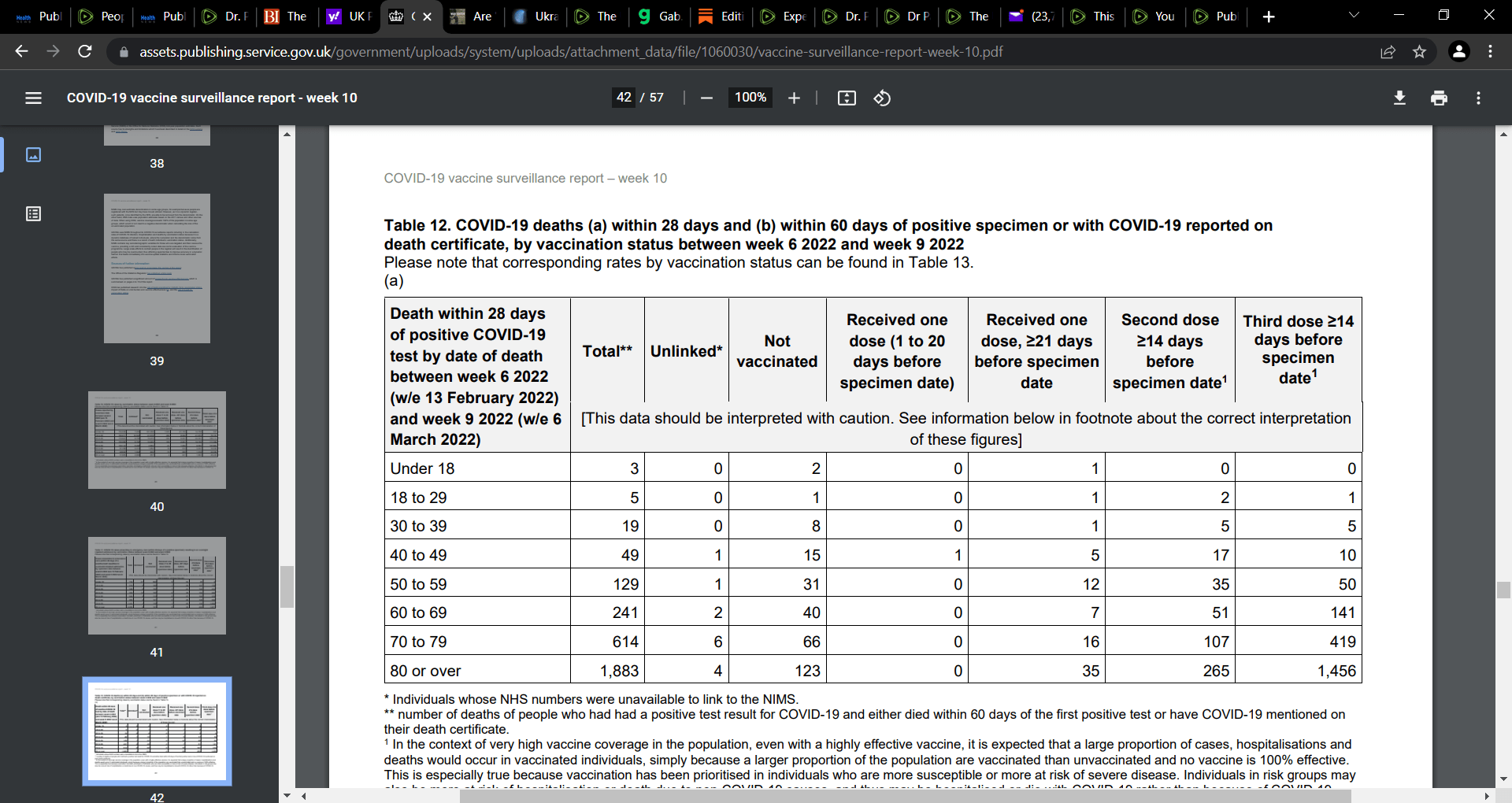
Predominant finding: vaccinated persons and especially for the 3rd booster shot, comprise approx. 90% of ER and deaths, relative to the unvaccinated. Getting vaccinated is not only causing you to become infected, but increases risk of severe outcome (hospitalization and death).
By vaccine status, we see the more shots, the greater the absolute cases
Hospital/ER, we see that the 2nd and 3rd shot is a problem with greater ER visits and this is very problematic for the 3rd booster, and particularly as age increases.
In terms of death, we see similar to the ER visits, that the more one is vaccinated and older ages e.g. > 50, that the risk of death escalates and dramatically e.g. in ages 18 and above, 90% of death occurs in those in receipt of vaccine compared to the unvaccinated. Similar is see for hospitalization/ER.
Now the week 10 compared to week 9 data:
Week 10:
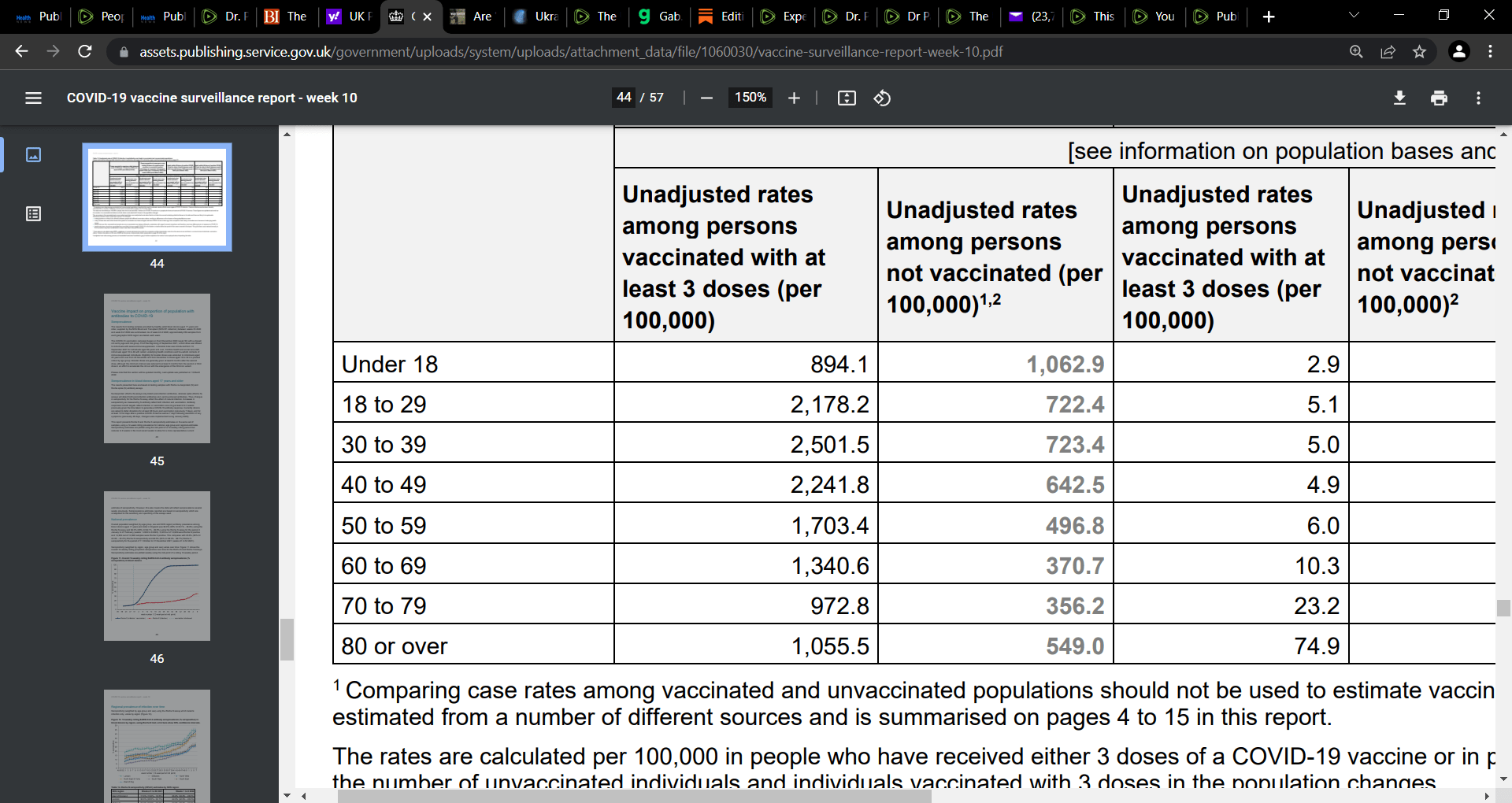
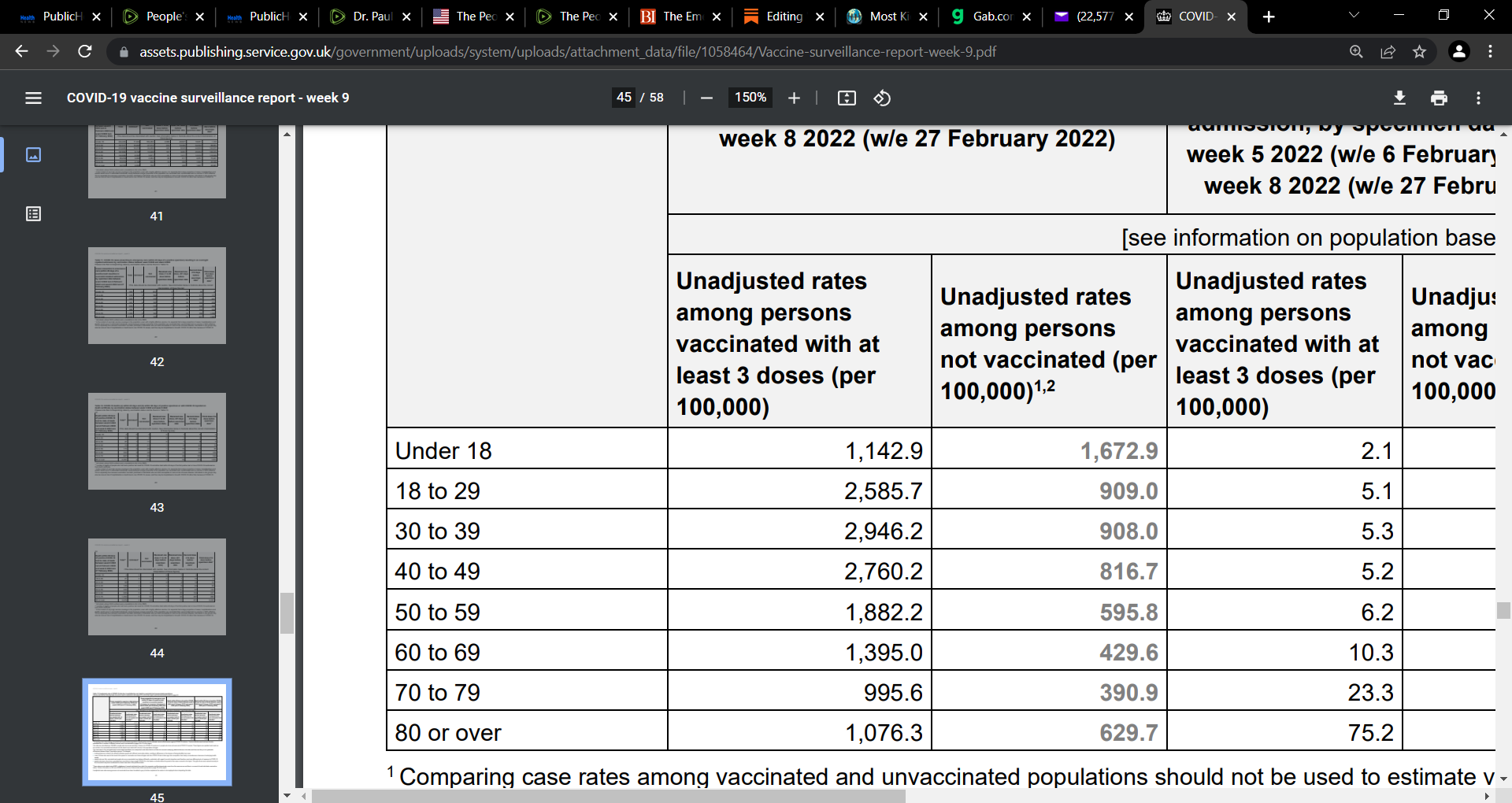
What do we see? We see as we saw across weeks 8, 7, 6, and 5 etc. that infection is decreasing in both the vaccinated and unvaccinated. We also see the much more elevated infection risk in the vaccinated above age 18 in week 9. Why this decrease in risk? One hypothesis is the role of the innate immune system:
-
in the vaccinated, there is regained functionality of the innate antibodies (Abs) since the vaccine does not confer sterilizing immunity and thus the vaccinal Abs can bind to the virus but not sterilize/neutralize (eliminate it/stop infection); the vaccine is to the initial legacy Wuhan strain and as such does not hit the predominant Omicron variant (spike). This resistance of the mRNA-induced vaccinal Abs to OMI, sets the innate Abs free that were prior outcompeted by the vaccinal Abs for the antigen (high specific high affinity vaccinal Abs vs broad, low affinity innate Abs). As such, given the resistance to OMI, the innate Abs can now function to sterilize the virus (eliminate it) and thus reduce infection and subsequent sequelae. This is one explanation to explain this data we are seeing.
-
In terms of the declining infection in the unvaccinated, this may be due to the learning or ‘training’ by the innate Abs across time in the unvaccinated, due to repeated exposure to the virus that is dominant and circulating. The unvaccinated are benefitting to the training of their innate immune systems and thus reduced infection across time. May explain why poorer less resourced nations with less aggressive vaccine programs have fared much better than those with elevated vaccine rates and aggressive roll-outs e.g. African nations etc. ‘Time’ assisted these nations. Less seemed to be the ‘equalizer’ and appears to be best and as such, nations that did not vaccinate aggressively and at high rates due to lack of resources, actually did better and the data shows this.
This is a hypothesis and its open to discussion and correction. But the declines cannot be explained by vaccine as the vaccine does not sterilize the virus and does not stop infection. So we need to think of the evolutionary dynamics and what is happening outside of the role of the vaccine and how mass vaccination in the midst of a pandemic is playing a role, a deleterious one with natural selection, especially in driving new infectious variants and potentially a lethal one. This is a nightmare situation and especially if we bring an OMI-specific vaccine. It will damage the present resistance of the vaccinal Abs to OMI and this can be catastrophic.
All this to say vaccines must stop and now! And never in children as this could damage their innate immune system and the potent innate Abs if as explained earlier, this is indeed the case, that innate has such a potent role. That is, if they are not subverted and allowed to function as they should.
Note, I know we are discussing raw data as to ER and death and we have not used the denominators, but this raw crude data is instructive nonetheless.