
EUGYPPIUS (excellent substack post): Covid suppressed influenza during the first years of the pandemic. This isn't a testing artefact, it's not a win for lockdowns and it doesn't make SARS-2 a special
by Paul Alexander
flu-eating supervirus. It does, however, suggest that non-pharmaceutical interventions to mitigate transmission and mass vaccination against endemic respiratory viruses are two very bad ideas.
The flu was substantially suppressed across much of the world for the first two years of the Covid pandemic.
Many, many people disagree with me on this point, more than ever before. While I’m generally happy to let ideas I think are wrong persist alongside my own point of view, this is an exception, because it touches on the phenomenon of viral interference, which is very real and very important.
Properly understood, viral interference calls into question the entire rationale for non-pharmaceutical interventions to slow the transmission of viruses, and suggests that mass vaccination against old endemic pathogens like influenza is a very bad idea – even in a fantasy world where those vaccines are absolutely safe, and especially if they’re in any way effective.
eugyppius: a plague chronicle is a reader-supported publication. maybe you subscribe?
Upgrade to paid
I want to be as clear about this as I can, so I’ll pull a Pueyo and tell you what I’m about to say before I say it:
-
I’m going to explain how we know influenza infections were heavily suppressed, especially in the first year of the Covid pandemic, from data that has nothing – zero – to do with mass pandemic testing.
-
I’m going to explain why viral interference is such a conceptual problem, and how it becomes easier to understand if we drop one of the core assumptions of epidemiology.
-
Finally, I’m going to suggest that ordinary endemic viruses are an important defence against potentially dangerous novel pathogens.
This is not a post about mass PCR testing and its reliability. Even without mass testing data, we have good reason to conclude that Covid coincided with the widespread suppression of influenza.
That said, it’s very important to acknowledge that influenza testing changed drastically after March 2020. Equally important is the fact that influenza was never diagnosed via mass PCR testing, as Covid was, and this makes it easy to get lost in meaningless apples-to-oranges comparisons. Furthermore, there is no denying that the raw number of flu tests fell nearly to zero for the entire space of the pandemic period. Finally, there existed in most jurisdictions considerable financial incentives for diagnosing Covid infection in as many patients as possible, especially when those patients died.
These points raise grave questions about the integrity of our pandemic-era influenza data, but they don’t make a positive case in either direction. In what follows, and for the sake of argument, I’ll assume that ordinary diagnostic influenza testing ceased the world over on 1 March 2020. I’ll assume that the WHO FluNet statistics and CDC numbers are hopelessly confounded.
Evidence for influenza suppression after 2020
I’ve made my case for what happened to influenza during the pandemic multiple times, and I suspect that none of you want me to rehearse that in detail ever again. If you are, however, interested in links to the data and closer discussion, please see this piece on the Mysterious Disappearance of Influenza and this piece on the phenomenon of viral interference.
Here I’ll simply spell out the main points. There are four of them:
1) Various jurisdictions have small self-contained influenza surveillance programmes. Mass Covid PCR insanity did not affect these programmes. In Germany, participating sentinel clinics swab patients with respiratory symptoms and send these swabs to a testing centre. During the pandemic, they tested each of these swabs for each of seven viruses: rhinoviruses, ordinary human-infecting coronaviruses, influenza, RSV, parainfluenza, human metapneumovirus and SARS-2. They’ve been doing this for a long time, yielding a wealth of data going back years about the seasonal patterns of the endemic viruses we live with. And this is the key point: After March 2020, influenza disappears entirely from German sentinel clinic swabs. Other viruses are heavily suppressed but not totally gone; only rhinoviruses seem unaffected.
eugyppius: a plague chronicle is a reader-supported publication. maybe you subscribe?
Upgrade to paid
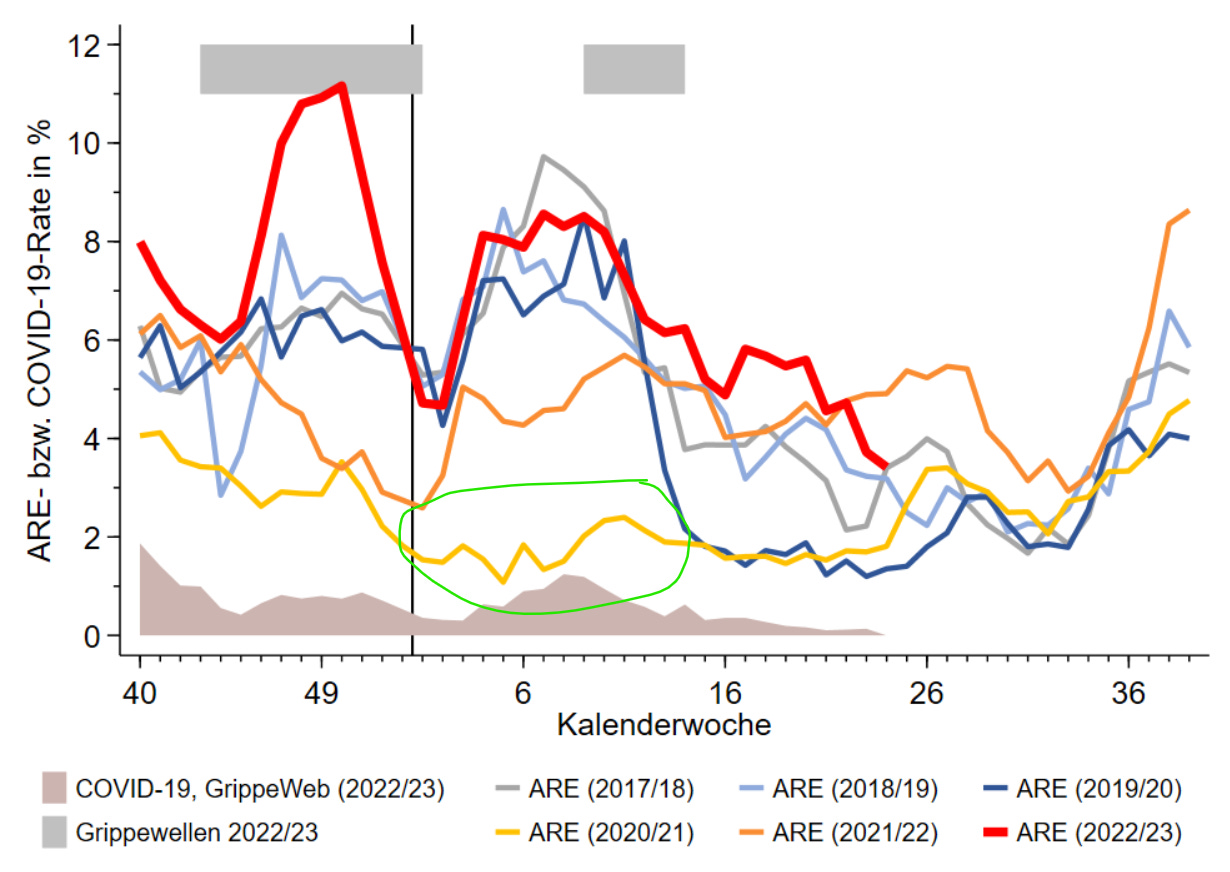
2) The behaviour of influenza, at the population-level, is seasonally distinct. In most places, flu infections peak in February or March. Rhinoviruses, by contrast, are most active in the fall and the spring, and other respiratory viruses are most prevalent around the winter solstice in late December. If influenza were merely rebranded as Covid or overlooked by the pandemic-era testing regime, we’d expect fever gauges like Grippe Web
to show the usual double-peak of virus respiratory systems, with one peak for the solstice viruses in December and another peak for flu after January. We don’t see that.For the crucial 2020/21 season, the post-January influenza peak is totally missing, and the solstice peak is anomalously low, in fact barely perceptible.This data is independent of all virus testing.
3) Very much in contrast to Covid and the other common respiratory viruses save RSV, influenza causes a small yet nontrivial number of hospitalisations and deaths in very young children. If flu were overlooked or rebranded as Covid during the pandemic, we’d expect to see the usual flu-related February/March hospitalisations and deaths in this age cohort, but we don’t. They’re totally missing. This is another data point totally independent of mass testing.
4) Viral interference is very real, and it has been observed for a long time. Some of the most convincing data emerges from studies of the 2009 Swine Flu. In this over-hyped “pandemic,” a new H1N1 flu strain spread across the globe, causing mild symptoms in most everyone. For humans, it was a nothinburger, but for the world of viruses, it was very disruptive, because viruses don’t have to be extra special or especially dangerous to upset the viral ecosystem. Ordinary human-infecting coronaviruses were heavily suppressed across the entire 2009/10 season. Almost nobody locked down for the Swine Flu, there was no mass PCR insanity, and yet multiple studies attest to a clear interference effect.
How viral interference probably works and why standard epidemiological assumptions are wrong
Viral interference does not – cannot – involve the direct competition of viruses within the same host. Only a small minority of the population (generally 2-10%) suffers symptomatic respiratory virus infection at any given time. Many influenza-shedding hosts will never encounter a single SARS-2-shedding host for the duration of their symptoms. And yet, viral interference happens.
What is going on?
Here it will help to consider all the other phenomena we’ve been treated to since 2020 that the virus understanders are equally powerless to explain:
-
How is it that waves of infection generally collapse of their own accord, well before burning through the entire population?
-
Why were non-pharmaceutical interventions, especially lockdowns, so powerless to do anything about Covid mortality?
-
And, above all, why were the virus models so invariably, irretrievably wrong all the time?
We are labouring under a serious error, and that error is to be sought somewhere in the SIR model of virus transmission. In the deceptively logical, simple world of SIR (which underpins not merely virus computer modelling but much epidemiological thought) immunologically naive people are held to be Susceptible until they encounter the virus. They are then Infected, after which they either die or Recover and are immune.
This model is particularly attractive to the vaccinators of the world, who believe that they can snatch people out of the Susceptible pool by jabbing them, and drop them into the Recovered/Vaccinated column, thereby skipping the dreaded Infected part.
Well, dear readers, we have endured an unprecedented exercise in mass vaccination. It had many effects on virus transmission, but none of it looked like SIR told us it would. Many theories are possible, but anyone who seriously attempts to understand how viruses actually behave must sooner or later throw SIR into the trash.
R. Edgar Hope Simpson, in trying to account for the many oddities of influenza transmission, effectively located the error of SIR in its overly simplistic conception of what it means to be Infected and Recovered.
As for Covid, SIR looks to be entirely too simplistic in its conception of the Susceptible. An ordinary population not subject to a multi-year Chinese hygiene regime has substantial resistance to viral infection in general. Scroll up and look at the German fever-gauge data once more. Note how, across the entire German population, symptomatic infections seem to have serious trouble breaching the 10% threshold. Whenever they scrape it, a collapse is imminent.
Here’s how I read that: Innate immune defences are powerful, and they make a solid majority of everybody invulnerable to respiratory virus infection at any given time. Viruses don’t have free run of the entire uninfected population; only a small minority of respiratory tracts are open to them. That Susceptible minority waxes and wanes with the seasons. In the summer, it’s very small indeed, and many viruses drop to nearly undetectable levels. In the winter, the number of Susceptible increases substantially.
We have a good explanation of viral interference, if we posit that prior infection with one respiratory virus knocks the recovered person out of the Susceptible column for many other viruses. Interferon is one likely mechanism here, but there are probably others. If you’re in the minority 5% susceptible and you get influenza, you’re most likely invulnerable to Covid for a while afterwards, and vice versa.
Once we revise our conception of who is susceptible, a lot of things come into focus. We wasted much effort locking down and vaccinating people who were invulnerable to infection in any case. This was entirely useless if not actively harmful, because Covid vaccination, it turns out, does not necessarily take you out of the susceptible column. On the contrary, it has bizarre and unexpected effects on virus susceptibility, often increasing it both in the near- and longer-term. Infection waves collapse well before they burn through the whole population because only a minority of people are susceptible at any given time. Models are wrong because they drastically overestimate susceptibility.
SIR, on closer consideration, is not an empirical attempt to understand virus transmission at all. Instead, it’s a heavily politicised paradigm, useful for exaggerating the threat of respiratory pathogens and justifying technocratic public health interventions like mass vaccination. It persists not because it’s right, but because it’s useful.
Ordinary endemic viruses are a defence against novel pathogens and lockdowns are very bad
The problem isn’t that lockdowns do nothing. It’s that they’re just effective enough to be dangerous. Endemic viruses that have been around forever face the standard constraints of seasonality and the drastic limitations our innate immune systems place on susceptibility, but they’re also boxed in by adaptive immunity. They face antibodies everywhere because they’ve been infecting billions of people since childhood. A newer pathogen, like SARS-2, faces fewer adaptive immune constraints.
When you lock down and put hand sanitiser on every corner, it’s the old endemic viruses that take the hit first. In preventing these infections, you effectively reserve precious susceptible respiratory tracts for the somewhat faster novel virus. We know that SARS-2 was circulating widely as early as Fall 2019, and yet it only coincided with serious mortality as influenza infections collapsed in the course of February and March.
The chronology suggests that influenza, already at the end of its season, was being out-competed in many places by Covid as early as February. Lockdowns are far from the only factor in play here, but everywhere the story is the same: Collapsing influenza is a precondition for pandemic mortality.

Influenza is far from the only virus with which SARS-2 competes. It’s almost surely no accident that SARS-2 was at its deadliest in heavily restricted care home environments. These were spaces in which a draconian hygiene interventions spared SARS-2 all competition. Compare the case of the Diamond Princess, where Covid also had access to a lot of old people but could rack up very few deaths, no doubt because of endemic virus competition.
Mass vaccination initiatives to reduce the prevalence of endemic respiratory viruses, including vastly milder Omicron-era Covid, are a very bad idea for the same reason that lockdowns are. Even if they’re totally safe, the risk is that they’ll end up reserving hosts for other, newer pathogens and the unknown risks that these pose.
eugyppius: a plague chronicle is a reader-supported publication. maybe you subscribe?
Upgrade to paid
At the end, a side matter: Influenza suppression in the absence of Covid
A common objection is that flu appeared to vanish in many regions that also had very few Covid infections in 2020, such as Eastern Europe and Taiwan. Thus, it is said, we must be dealing with artefacts of testing or behavioural changes rather than a real biological phenomenon.
The problem with this view, is that influenza has many unique characteristics that set it apart from other viruses. In some respects, it seems to behave like one pan-regional viral super-organism, evading human immunity via constant mutation and reassortment in millions of hosts. When it’s denied these substantial reservoirs, it suddenly faces significant disadvantages everywhere.
In the past, I’ve written of the “disappearance” of influenza, but here I’ve tried to speak more precisely of its suppression. Mass flu testing in 2020 would’ve undoubtedly uncovered cases across the world, and perhaps it would’ve even uncovered somewhat more cases in places where Covid was less prevalent. However that may be, it’s important to emphasise that influenza merely seemed to disappear, because it was not prevalent enough for our (often rather crude) flu surveillance programs to detect. (Some combination of Covid competition and pandemic restrictions does seem to have wiped out the Yamagata strain of Influenza B forever, though.)’
