
MUCOSAL immunity & why breakthrough infection in vaccinated individuals may result from lack of 'local' respiratory/mucosal protection; infectious pressure, vaccinal immune pressure, INNATE immunity
by Paul Alexander
I will argue anyone this, the vaccine could have never worked based on a design flaw; some would even ask, were these vaccines designed to fail and hung around Trump's neck had he had a 2nd term????
The core argument is that we underestimated the capacity of the vaccinal antibody immune pressure to impact the evolutionary capacity of the virus, and as such, for the virus to evolve and adapt. And it has. And if we do not stop this INSANE vaccine program with failed non-sterilizing vaccines that DO NOT stop transmission, then we will have more variants and the danger is one can be pathogenic and can even threaten humanity’s existence. It is that grave. Dr. Geert Vanden Bossche is correct. He is a friend of mines. A beautiful man. I am studying immunology and virology advancements under him now to address this debate.
Bottom line, by replacing innate immunity antibodies and acquired immunity antibodies with vaccinal antibodies, this will be disastrous and we will never ever get to population-level herd immunity with these non-sterilizing vaccines that cannot neutralize the virus. It is the mass vaccination into a pandemic using a non-sterilizing vaccine as these COVID vaccines that is driving the variants. We cannot discuss this without the Mortal antigenic sin phenomenon (you know as the original antigenic sin (OAS)) given folk like Dr. Dan Stock and I have postulated that the escalating infections post vaccination is due to the sub-optimal initial priming of the immune response, prejudiced toward systemic vaccinal antibodies and not the correct localized cytotoxic cellular response in the nasal mucosae. I will write separately.
What do we have here? The virus has responded by mutating on the spike that is a clear mismatch to the initial Wuhan spike. The vaccine just simply cannot work as the current vaccinal immunity does not hit the Delta and Omicron spike. Period. The vaccine does not work for OMICRON, in any manner. Nothing.
The public health officials and vaccine developers do not wish to admit failure but the fact is that the vaccinal immunity CANNOT hit the existing spike and this is the core thesis of why the vaccines have failed and will continue to and will drive immune escape. This is a very dangerous situation especially if we target our children as we will damage a fully functional innate immune system via the vaccinal antibodies. This is key.
Do we have any evidence that these vaccine can have severe consequences?
Yes, ‘we do have accumulating evidence and recent work by Seneff et al. shows us how much. There is ‘profound impairment in type I interferon signaling, which has diverse adverse consequences to human health. We explain the mechanism by which immune cells release into the circulation large quantities of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites. We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance. These disturbances are shown to have a potentially direct causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, increased tumorigenesis, and DNA damage.’ This is very important for us to consider.
https://www.authorea.com/doi/full/10.22541/au.164276411.10570847/v1
I wish to deal specifically with the issues: i) the issue the the mucosal immune system and how the vaccinal antibodies cannot reach/hit the mucosal lining/layer/barrier ii) vaccinating during a pandemic with massive infectious pressure up against mounting ‘sub-optimal’ vaccinal immune pressure and the role of natural selection is selecting the ‘fittest’ variants and iii) the innate immune system, with a focus on children and young persons, but particularly the innate antibodies of the innate immune system. Note, the natural innate immune system and the natural acquired-adaptive immune system are actually under the umbrella ‘natural immunity’. These two comprise natural immunity and in my understanding work together (in some manner overlap) to sterilize the pathogen/virus. I am not a virologist or immunologist yet I am sharing my understanding if it may help. I love sharing and learning. OK, lets go:
i)Mucosal immune system and these COVID vaccines (https://www.ncbi.nlm.nih.gov/books/NBK27169/)
The nasopharyngeal mucosa is the site of entry of SARS-CoV-2 virus. The vaccinal antibodies are in the blood stream while the initial infection is in the nasopharyngeal mucosa. This is the key to the argument of why the vaccines have, and are, and will fail. These vaccines. IMO, and based on how I understand the mechanics at play here. The vaccinal antibodies in this vaccine model do not get at the mucosal layer where it is needed and where the virus lands. When we are infected with SARS-CoV-2 (coronavirus) or similar respiratory pathogen, the virus will remain localized to the respiratory tract. Problem is that the vaccines cause an immune response that is systemic (post spike protein production by our cells).
There is very cogent and plausible explanations by Bhakdi that the vaccine fails out of the gate because it does not hit the mucosal layer where the virus resides initially. The mucosal barrier gives us protection against particularly respiratory viruses, and when the mucosal barrier/lining is stimulated based on virus landing there (e.g. in your nostrils/nasopharyngeal passage), the mucosal barrier/lining ramps up a response on the virus and cues the immune response internally for battle.
In other words, the optimal inoculation, the best vaccine that was needed for COVID was one that stimulated the mucosal barrier (e.g. nasal spray vaccine delivering antigen there). By applying a muscular injection at the deltoid using the COVID vaccines e.g. mRNA, this would not stimulate the mucosal barrier and thus will not drive the proper immune response. This is the problem here. Bhakdi et al. argue the vaccine never worked and could never work in the first place. These vaccines, based on the design, and he was not even talking yet about the toxic side effects and harms. Thus these can never work for children based on what we just said.
Maybe this is what Dr. Robert Malone refers to by Omicron being nature’s vaccine, as it lands in the nostrils/mucosal barrier (respiratory tract) and drives the immune response at the mucosae. With no toxic side effects and mild symptoms if any and with recovery. Then immunity. We can even get in there early and introduce nasal and oral wash outs to clean out the virus and prevent it taken hold.
Was this design flaw a deliberate one? Why would we not have made a vaccine that targeted the mucosal barrier?
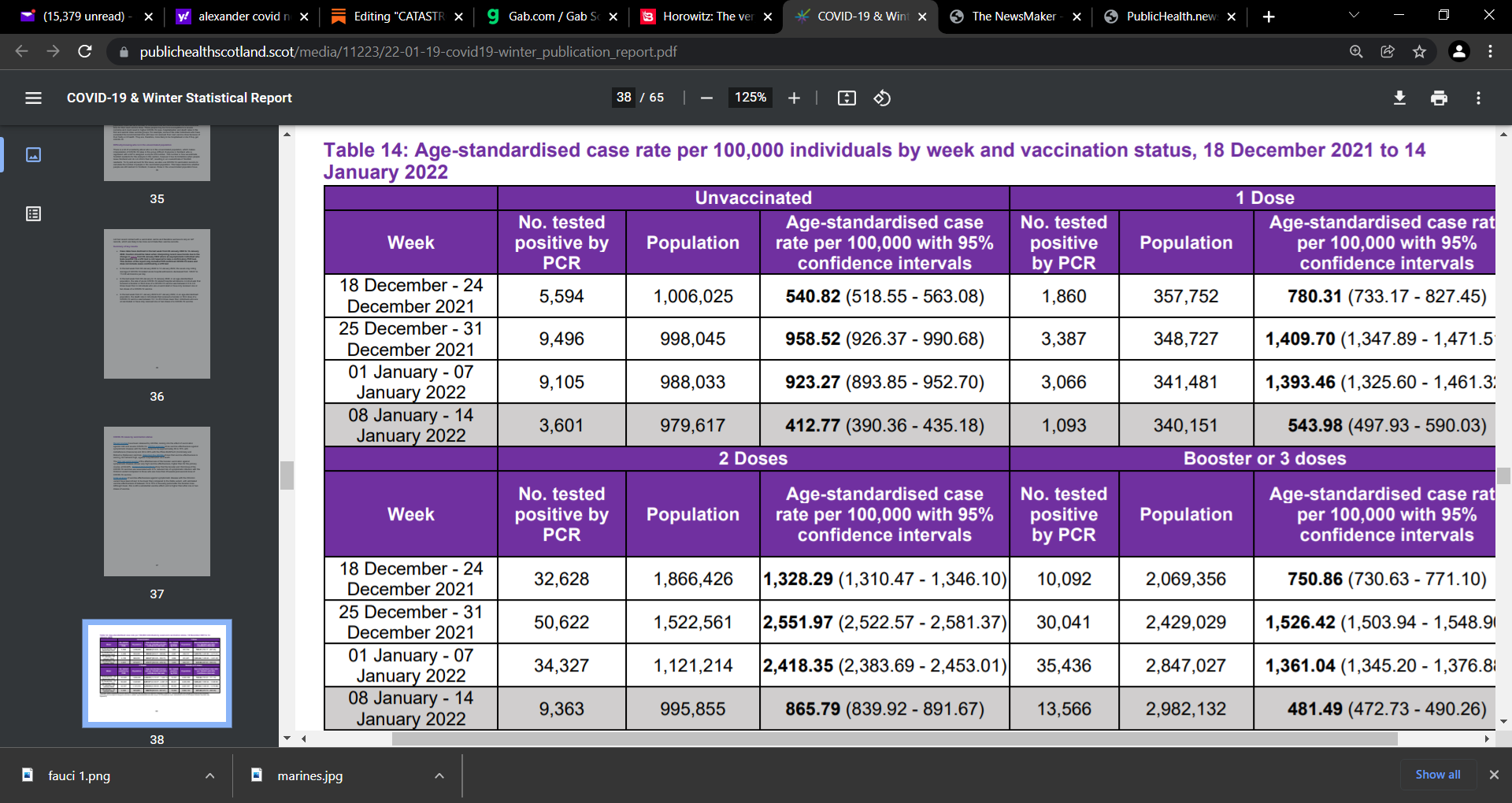
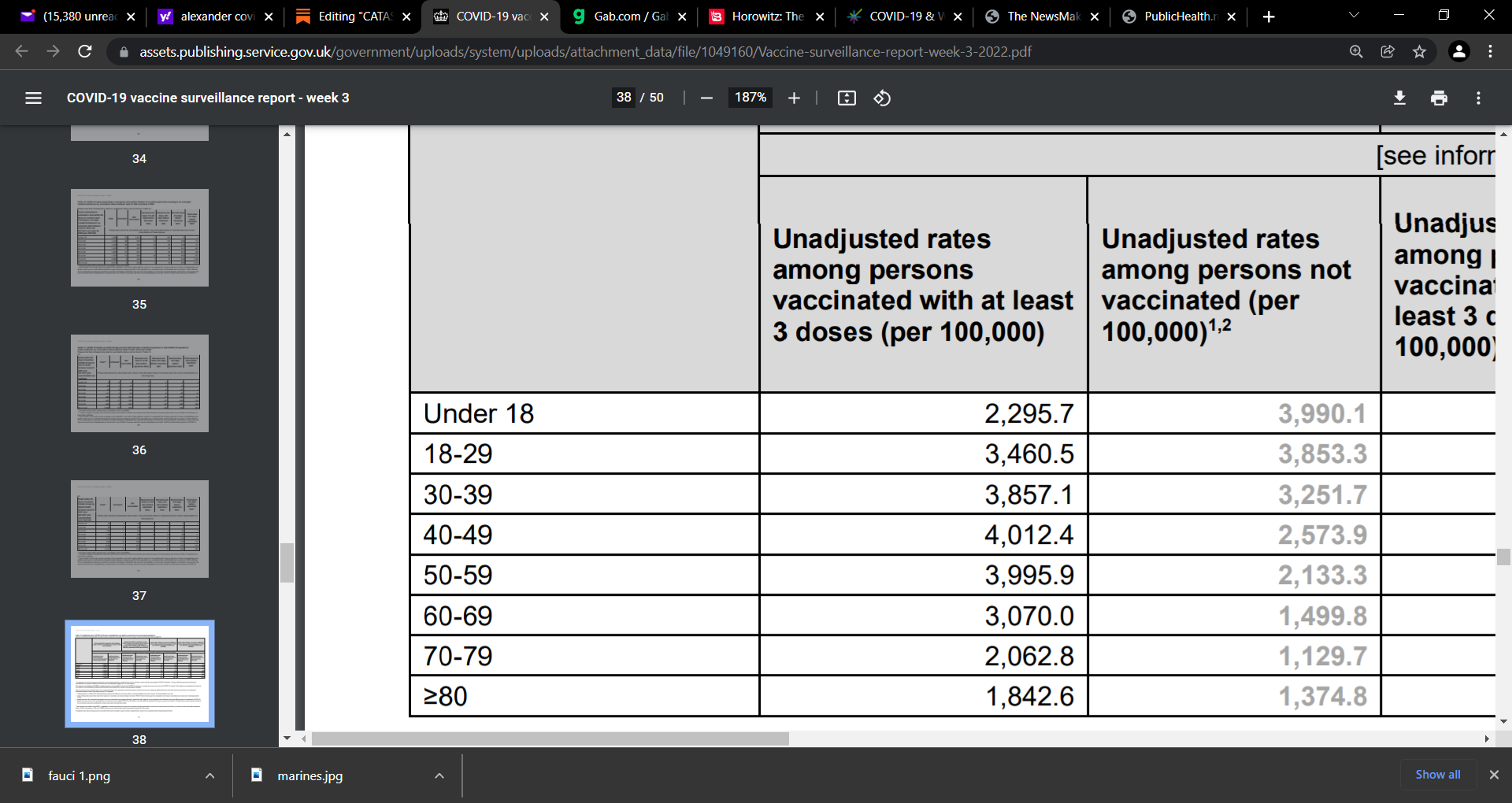
At this time based on all we know, I argue no one should get a COVID vaccine, no 2nd shot, no booster, NONE! The data now is clear and the recent UK and Scottish data shows us this.
Scottish:
UK:
Also, look at the massive risk of myocarditis reported by Oster et al in JAMA:
Oster et al. JAMA doi: 10.1001/jama.2021.24110.; risk of MYOCARDITIS after receiving mRNA-based COVID-19 vaccines is increased across multiple age & sex strata & highest after second vaccination dose
192,405,448 persons receiving a total of 354,100,845 mRNA-based COVID-19 vaccines during the study period, there were 1,991 reports of myocarditis to VAERS & 1,626 of these reports met case definition

Now for the core thesis:
You can only control a pandemic if you can control and cut the chain of transmission. If you cannot cut the chain, then you will never ever get to herd immunity and these COVID vaccines do not cut the chain of transmission, they do not sterilize the virus. They do not stop transmission and thus it makes moot the issue of vaccine mandates.
Again, DO NOT vaccinate with these vaccines under any condition now. None!
Do not vaccinate under any condition with these vaccines.
We greatly underestimated the impact of the mass vaccination on the evolutionary capacity of the virus to evolve to the pressure. It is the mass vaccination using a non-sterilizing vaccine (that does not stop infection or transmission) and in the midst of an ongoing pandemic that is causing the emergence of variants.
There is massive infectious pressure from the circulating virus. There is massive pressure from the vaccinal antibodies (though sub-optimal and not very strong as not yet mature) directed on the spike itself, the receptor binding domain. Pressure on the infectiousness of the virus.
The pressure also is on one of the most neglected components of immunity, the INNATE immune system, which is also a component of natural immunity. The innate immune system responds to novelty potently, and is the initial immune defense children and young persons have. It protect children against a broad range of pathogen. The innate immune system can be damaged by COVID vaccines.
The major issue is the underestimation of the impact of mass vaccination and the wide spread population immune pressure on the evolutionary capacity of the virus to evolve, and escape the immune response (viral immune escape). Yes, there is immune pressure on the first line of defense, the innate immunity. We have to immediately stop this immune pressure (via vaccinal antibodies) on the virus and innate immunity for it is incapable of blocking transmission. Yet placing the virus under pressure.
GVB explains that it is not a problem to vaccinate the vulnerable at-risk portions of society. It is the mass vaccination that creates a disaster and is harmful. It is a catastrophic failure to put massive immune pressure while you do not block transmission. This can lead to other diseases due to suppression of the innate antibodies by the vaccinal antibodies. If the innate antibodies are suppressed (outcompeted) by the vaccinal antibodies, then this can cause other illnesses to emerge, especially in children. The innate antibodies can be outcompeted for binding by the vaccinal antibodies because they are non-specific and of low affinity while the vaccinal Abs are high-affinity and very specific for the antigen.
The concern also is that vaccinal antibodies are boosted while having a highly infectious variant circulating and the likely hood of exposure and re-exposure and then boosted and boosted and with this, there is a continuous suppression of innate immunity.
GVB has explained that the resistance of omicron to the vaccinal antibodies is a good thing because it no longer can outcompete the innate antibodies and this sets the innate immunity free to sterilize the virus.
Children are the main concern as innate antibodies are potent but weak in the sense that they could be outcompeted by vaccinal antibodies. If that happens, we would then deny them their potent innate immune response, for a broad range of pathogen
Some have great innate immunity and they get exposed and their innate (antibodies and NK cells) can neutralize the virus and the virus will not even get into the cells. You have no symptoms etc. Others have mild symptoms as virus may get into the cells but you will experience a little mild illness for a few hours or a day and then recover. Then in others, virus can break thorough innate to the acquired-adaptive compartment and will be neutralized there. If virus breaks through the innate line of defense, the innate would have mitigated the virus and has taken the edge (so to speak) off so that the acquired-adaptive portion of immunity can then deal with the virus. GVB explains that without the innate, the acquired-adaptive natural immunity could be overwhelmed by the virus. Thus you should not discuss one without the other.
There is both the antibody and the cellular (NK cells) components (and others) of the innate immunity, as if for the acquired-adaptive natural immunity. Both the innate and the acquired-adaptive components work together to eliminate the virus.
If vaccinated, and these COVID non-sterilizing vaccinal antibodies suppress and replace innate antibodies that could have neutralized the virus, then the chain of transmission cannot be cut and we will never get to population-level herd immunity. By non-sterilizing sub-optimal ‘immature, not fully developed’ vaccinal antibodies binding but not sterilizing the virus, then the innate are blocked from binding, and thus unable to sterilize and prevent infection.
So at the end of the day, we are creating a disastrous situation whereby we are converting people with strong potent, functional innate and acquired natural immunity, and by vaccinating them, into persons with immunity that cannot stop transmission and this breaks herd immunity.
I am saying no vaccine, not even in vulnerable people. Based on all we know now of these vaccines.
Bottom line, by replacing innate antibodies and acquired antibodies with vaccinal antibodies, this will be disastrous and we will never ever get to herd immunity with these non-sterilizing vaccines that can not neutralize the virus.